take a seat
The Smart Seat is an effortless in-home wellness tracker. It replaces your toilet seat and quietly reads your vital signs every time you sit. No wearing, no charging, nothing new to learn.
A decade of clinical research · No camera, no microphone · Made in Rochester, NY
Staying ahead of your health shouldn't feel like a part-time job.
Cuffs, clips, charging cables, and gadgets you have to remember to wear. Most people give up.
Three steps. Then never think about it again.
Swap your seat.
A simple install in minutes. It looks and works like a normal toilet seat.
Just sit.
Every time you sit, the Smart Seat reads your vitals in under two minutes. Nothing to wear, nothing to charge, nothing to remember.
See your normal.
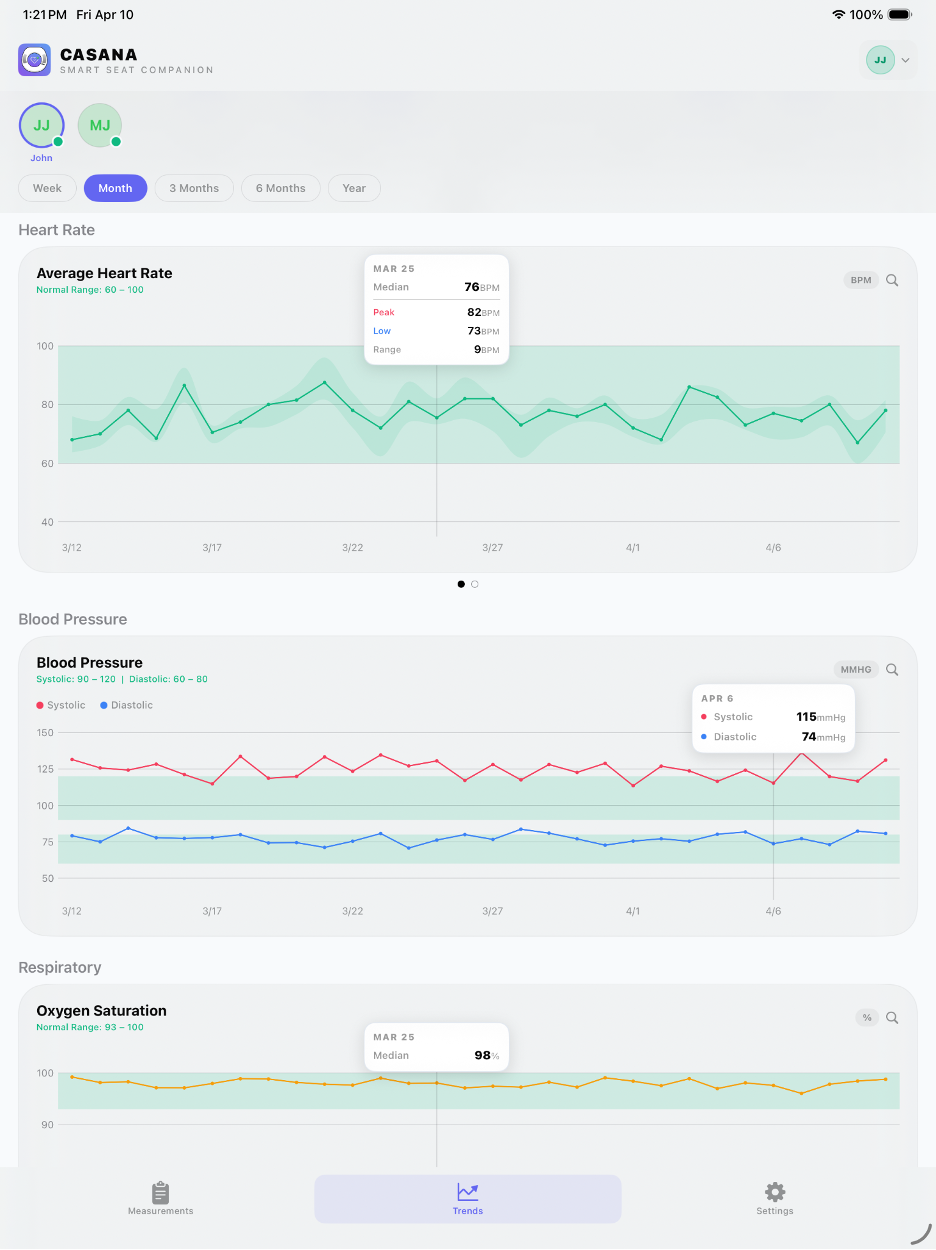
Your readings appear as simple trends in the app. Get a gentle heads-up when something looks different from your normal, and share with family or your doctor only if you choose.
A few sits a week is enough to track your trends. There's nothing to keep up with.
A full read on the vitals that matter.
Heart rate & HRV · Blood oxygen (SpO₂) · Respiration · Blood-pressure trends · Everyday patterns (your routine).
Built on a decade of research.
Clinical research (including an arterial-line study), 3rd party validation studies, international patents, and serious backers: General Catalyst, Matrix, Morningside, Outsiders, Kaiser Permanente, and Bemis (the world's largest toilet-seat maker) behind every reading. Designed and made in Rochester, New York.
No camera. No microphone. Your data is yours, shared only if and when you choose.
Shown as trends against your own normal. For wellness, not diagnosis.
Loved by Thousands
Join our community of Smart Seat enthusiasts.
"This is the Apple Watch for seniors."
Sarah M.
"Knowing if my mom has abnormal patterns jump out is so helpful. It gives me peace of mind without having to constantly check in on her."
David L.
"The Stability feature is a new one. I haven't seen that before and it's been very interesting to see where I stand (or sit!)."
Jennifer K.
Ready to Sit?
$199 to start. Everything you need for your first year.

Smart Seat + your first full year of service
Early Bird Special
- Free Shipping
- Up to 5 household members included
- Wellness Suite
- Stability Suite
- Habits Suite
- Caregiver and Family Sharing Enabled
- Wi-Fi enabled
- Soft-close lid
- 3-year warranty
- 30-day money-back guarantee
Secure checkout powered by Shopify & Stripe.
After your first year, service continues at $19.99/month. Cancel anytime; the seat is yours.
Frequently Asked Questions
Everything you need to know about Smart Seat.
Stay ahead of your health, right where you already are.
Looking for the Smart Seat Companion App?
The Smart Seat is a wellness device for general monitoring. It is not intended for medical use.
We use cookies
We use Google Analytics to understand how visitors use our site so we can improve your experience. No personal data is sold. You can accept or decline analytics cookies; essential site functions always remain active.