take a seat
The Smart Seat is the world's first smart toilet seat that quietly tracks everyday wellness (vital signs) right where life already happens, in the comfort of your home. Same routine. Smarter insights.
Why Choose the Smart Seat?
You don't need to turn anything on, charge anything up, or change your routine. Just use the toilet like you always do, we'll take care of the rest.
Blends into the Background
Nothing to charge. Nothing to remember.
Wellness Insights
No guessing. Just helpful patterns.
Data Privacy
Your data is encrypted and never shared with third parties without your permission.
Support your Independence
Keep your loved ones and / or your health care provider informed.
Engineered for Excellence
Grounded in over ten years of scientific research alongside world-renowned institutions, the Smart Seat quietly monitors your everyday wellness signals.

Everyday Wellness Monitoring
The Smart Seat works in the background, quietly tracking key wellness signals like heart rate, blood oxygen levels, stability, and blood pressure so you can spot meaningful changes early.
- Heart rate monitoring
- Blood oxygen level tracking
- Stability analysis
- Blood pressure insights
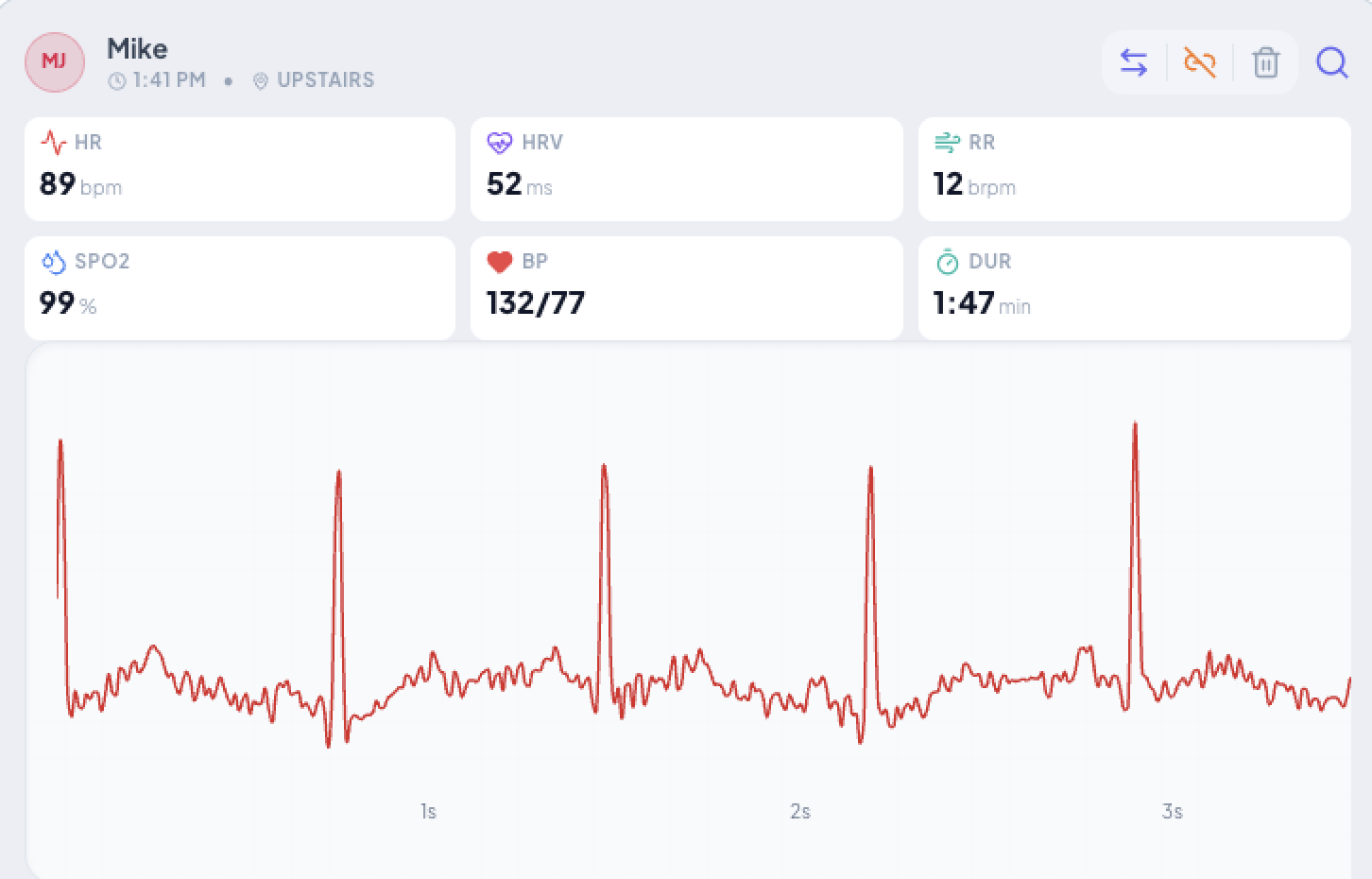
Clear Insights
The Smart Seat dashboard uses clean, simple visuals to highlight vital signs over time, making it easy to understand wellness trends and notice changes from your mobile device or on the web. Easy to share healthcare trends with loved ones and health care providers.
- Clean visual trends
- Normal vital signs ranges
- Access your data on your mobile device or web browser
- User can elect to share data with loved ones and / or caregivers

Data Privacy
Your health data belongs to you. All biometric measurements captured by the Smart Seat are encrypted, never sold to third parties, and stored in accordance with the highest industry privacy standards.
- The Smart Seat uses bioidentification to recognize different users in the household
- Individual user data is private and encrypted
- Data sharing with loved ones and or caregivers is in your control
- For more information see casanacare.com/privacy-policy

Simple Installation & Connectivity
The US standard double bolts (yes, one thing the whole country agrees on) easily installs the Smart Seat on your elongated toilet. A simple setup process connects your Smart Seat to your wifi.
- Simple, standard two-bolt installation
- Only fits elongated toilets (see casanacare.com/compatibility for a compatibility guide)
- Easy wifi setup
- No special care or cleaning of the seat required
_1768245904793-DYye6pJP.jpg)
Embedded Sensors
Three unique sensors are embedded in the Smart Seat: single-lead electrocardiogram (ECG), photoplethysmogram (PPG) and load cell derived ballistocardiogram (BCG).
- Single-lead ECG
- Photoplethysmogram (PPG)
- Ballistocardiogram (BCG)
The ultimate wellness gift for a loved one
Peace of mind, without hovering.
Stay connected to your loved ones' wellness without intruding on their independence.
Loved by Thousands
Join our community of Smart Seat enthusiasts.
"This is the Apple Watch for seniors."
Sarah M.
"Knowing if my mom has abnormal patterns jump out is so helpful. It gives me peace of mind without having to constantly check in on her."
David L.
"The Stability feature is a new one. I haven't seen that before and it's been very interesting to see where I stand (or sit!)."
Jennifer K.
Ready to Sit?
Same routine. Smarter Insights.

Smart Seat + 1 year of data
Early Bird Special
- Free Shipping
- Household members included
- Wellness Suite
- Stability Suite
- Habits Suite
- Caregiver Enabled
- Wi-Fi enabled
- Soft-close lid
- 3-year warranty
- 30-day money-back guarantee
Secure checkout powered by Stripe
Frequently Asked Questions
Everything you need to know about Smart Seat.
Stay in the Loop
Looking for the Smart Seat Companion App?
We use cookies
We use Google Analytics to understand how visitors use our site so we can improve your experience. No personal data is sold. You can accept or decline analytics cookies; essential site functions always remain active.